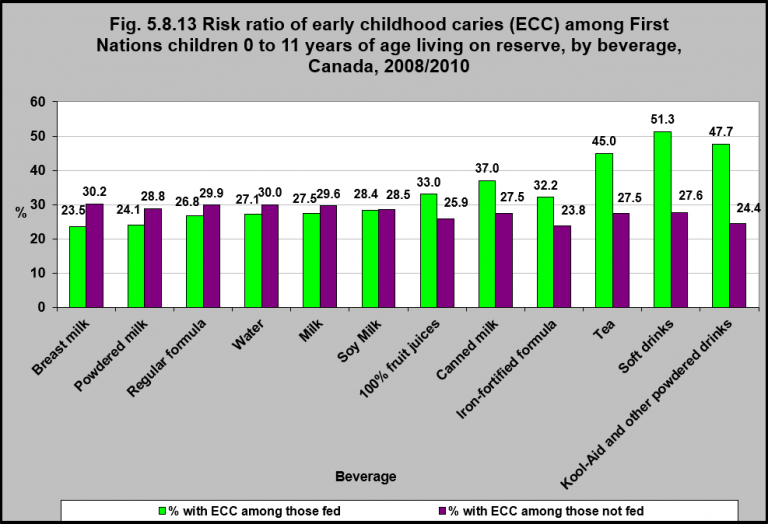
Risk ratio of early childhood caries (ECC) among First Nations children 0 to 11 years of age living on reserve, by beverage, Canada, 2008/2010
Note:
As reported by primary caregivers.
Source: CICH graphic created using data from the First Nations Regional Longitudinal Health Survey (RHS) 2008/10, National report on adults, youth and children living in First Nations Communities. https://fnigc.ca/sites/default/files/docs/first_nations_regional_health_survey_rhs_2008-10_-_national_report.pdf -accessed August 2, 2017.
In 2008/2010, First Nations children aged 0 to 11 living on reserve who drank fruit juices, canned milk, iron-fortified formula, tea, soft drinks and powdered drinks were at greater risk of developing early childhood caries** (ECC) than those who did not consume these beverages.
The potential risk of these beverages is concerning with over 50% of First Nations, Métis and Inuit children aged 2 to 5 years consuming two or more servings of soft drinks and/or juice each day.1
According to the 2007/2008 Nunavut Inuit Child Health Survey2, on average 78% of children aged 3-5 consumed 3 glasses of sweet drinks daily which equals approximately 30 sugar cubes.2
The figure for Nunavut Inuit children was over 7 times the national average for children aged 1-3 years and over 3 times the national average for children aged 4-8 years.3
For more information please see the Early childhood tooth decay factsheet developed by the National Collaborating Centre on Aboriginal Health and the Canadian Paediatric Society’s Position Statement on Early Childhood Caries in Indigenous Communities.
**Early childhood caries (ECC) is defined as the presence of tooth decay involving any primary tooth in a child younger than six years of age.4 ECC is also referred to as early childhood tooth decay in the vernacular (and formerly called baby bottle tooth decay).5
12006 Aboriginal Children`s Survey. http://www.statcan.gc.ca/pub/82-003-x/2013004/article/11776-eng.htm-accessed August 24, 2017.
2The International Polar Year Nunavut Inuit Child Health Survey 2007-2008. http://www.inuithealthsurvey.ca/pdf/Child_Inuit_Health_Survey_Aug_31.pdf-accessed August 5, 2017.
3Garriguet, Didier. Beverage consumption of children and teens. 2008. Component of Statistics Canada Catalogue no. 82-003-x. Health Reports. http://publications.gc.ca/collections/collection_2008/statcan/82-003-X/82-003-x2008004-eng.pdf– accessed August 10, 2017.
4American Academy of Pediatric Dentistry. Definition of early childhood caries (ECC). Pediatr Dent 2005;27(7 Reference Manual):13. http://www.aapd.org/media/policies_guidelines/p_eccclassifications.pdf– accessed July 12, 2017.
5Position Statement – Early Childhood caries in Indigenous communities. 2016. Canadian Paediatric Society. JD Irvine, S Holve, D Krol, R Schroth; Canadian Paediatric Society , First Nations, Inuit and Métis Health Committee. http://www.cps.ca/en/documents/position/oral-health-indigenous-communities-accessed August 2, 2017.
Implications
Bottle feeding babies sugary liquids during sleep is one of the most prominent causes of tooth decay among children.6 Bacteria in the mouth uses sugars from liquids such as milk, juice and formula, to produce acids which decay the teeth. Indigenous children are more susceptible to early childhood caries (tooth decay in children less than 6 years) because many live in rural and remote or northern communities where drinking water often has not been supplemented with fluoride, as well as because of limited access to preventive care and dental services.6
6BC Aboriginal Childcare Society. (2007). Aboriginal children and early childhood caries (ECC). West Vancouver, BC: Author. Retrieved October 11, 2017 from http://www.acc-society.bc.ca/files_new/documents/CFOCFebApr07.pdf