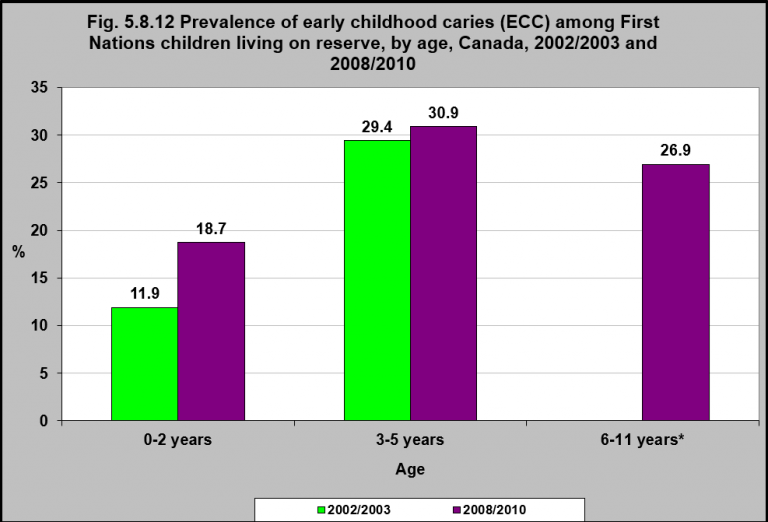
Prevalence of early childhood caries (ECC) among First Nations children living on reserve, by age, Canada, 2002/2003 and 2008/2010
Notes:
*Early childhood caries prevalence estimates for children aged 6 to 11 years were not reported in the Regional Health Survey 2002/03.
Early childhood caries was formerly called baby bottle tooth decay.
Source: CICH graphic created using data adapted from the First Nations Regional Longitudinal Health Survey (RHS) 2008/10, National report on adults, youth and children living in First Nations Communities. https://fnigc.ca/sites/default/files/docs/first_nations_regional_health_survey_rhs_2008-10_-_national_report.pdf -accessed July 17, 2017
Early childhood caries (ECC) is defined as the presence of tooth decay involving any primary tooth in a child younger than six years of age.1 ECC is also referred to as early childhood tooth decay in the vernacular (and formerly called baby bottle tooth decay).2
In 2008/2010, the prevalence of early childhood caries (ECC) among First Nations children living on reserve aged 0 to 2 was 18.7%. It was 30.9% for 3 to 5 year olds.
The prevalence of ECC for all age groups increased from 2002/2003 to 2008/2010 (except for the 6-11 age group, which was not reported in 2002/03).
According to the Inuit Oral Health Survey Report (2008-2009), over 85% of preschoolers reported dental caries with a mean of 8.22 deciduous (baby) teeth affected. By the time of adolescence, 97.7% had been affected. The prevalence greatly exceeded similar counts for southern Canadians.3
Multiple studies have shown that Indigenous children are disproportionately burdened by ECC.4
For more information, see the Early childhood tooth decay factsheet developed by the National Collaborating Centre on Aboriginal Health and the Canadian Paediatric Society’s Position Statement on Early Childhood Caries in Indigenous Communities.
1American Academy of Pediatric Dentistry. Definition of early childhood caries (ECC). Pediatr Dent 2005;27(7 Reference Manual):13. http://www.aapd.org/media/policies_guidelines/p_eccclassifications.pdf-accessed August 3, 2017.
2Position Statement – Early Childhood caries in Indigenous communities. 2016. Canadian Paediatric Society. JD Irvine, S Holve, D Krol, R Schroth; Canadian Paediatric Society , First Nations, Inuit and Métis Health Committee. http://www.cps.ca/en/documents/position/oral-health-indigenous-communities-accessed August 30.
3Inuit Oral Health Survey 2008 – 2009. Health Canada, 2011. http://www.hc-sc.gc.ca/fniah-spnia/alt_formats/pdf/pubs/promotion/_oral-bucco/oral-inuit-buccal-eng.pdf-accessed August 10, 2017.
4National Collaborating Centre for Aboriginal Health. 2013. Early Childhood Tooth Decay. http://www.nccah-ccnsa.ca/Publications/Lists/Publications/Attachments/95/Tooth_Decay_EN_web.pdf-accessed July 10,
2017.
Implications
Tooth decay, exemplified by the high prevalence of early childhood caries (ECC), is a major child health issue for Indigenous children. ECC can contribute to adverse health effects, including altered chewing, eating and sleeping patterns due to pain; potential growth restriction; speech difficulties; low self-esteem, and poor bite.5 It has also been associated with infectious diseases like respiratory tract infections and acute otitis media, as well as with obesity in children with families of low socioeconomic status, though possibly from common risk factors. Rates of ECC have been reported to be 86% among First Nations 3-5 year olds,6 with rates exceeding 90% in some Indigenous communities.5 Severe ECC frequently requires extensive treatment under general anesthesia, which can be costly for Indigenous families living in rural and remote communities who may not have access to dental surgery services. Dental surgery for severe ECC is common among Indigenous children, and recent studies suggest that a significant number of First Nations children with dental caries require repeat dental procedures under general anesthesia.5 Common risk factors for ECC include poverty, which is prevalent among First Nations children, as well as prolonged use of the bottle or training cups containing sugary drinks and high consumption of sugary snacks. Given the challenges and costs of surgical treatment of ECC in remote Indigenous communities and the fact that relapse and recurrent decay are common in such communities, dental disease will not be solved in Indigenous communities without disease prevention strategies that emphasize not only the preservation of healthy teeth, but also emphasize community development and address the determinants of health.
5Irvine, J.D., Holve, S., Krol, D., Schroth, R., & the Canadian Paediatric Society, First Nations, Inuit and Métis Health Committee. (2011). Early childhood caries in Indigenous communities: Position statement. Paediatric Child Health, 16(6), 351-7.
6First Nations Information Governance Centre. (3023). Report on the findings of the First Nations Oral Health Survey (FNOHS) 2009-10. Ottawa, ON: Author.